The escalating risks associated with the illicit use of adversarial AI in today’s world are difficult to overstate. Criminal syndicates have long been warehousing assorted intercepted data (including stolen personal health information), gambling that quantum computing will eventually mature enough to salvage a fraction of its value.
Now, they’re also deploying adversarial LLMs and agentic AI. As if this weren’t enough, the average HIPAA violation settlement in 2025 so far is over $342,000. In this landscape, the imperative to continuously and consistently safeguard patients’ medical data has never been more urgent. The risks faced by practitioners and institutions are not only exponentially greater in scale but qualitatively transformed. New threats are emerging that disguise the oldest tactics, yet new allies have also entered the field – including agentic AI.

The compliance illusion
In regulated healthcare environments, the word “compliance” has become a kind of security talisman: cited often, understood vaguely at best, and relied upon far beyond the scope of its actual protective power. Breaches continue to escalate both in numbers and severity, and settlements continue to climb, even among organizations that passed their most recent HIPAA audit. That dissonance reveals a dangerous truth: compliance is not protection. Audit checkboxes do not equal reducing real operational risk. Far too often, what looks secure on paper is quietly vulnerable in practice.
This illusion of safety is perpetuated by treating HIPAA as a periodic audit event; a hurdle to be cleared, rather than a system of obligations to be lived. When teams orient their processes around pass/fail criteria instead of dynamic threats, they mistake visibility for effectiveness. Controls exist, but they may be outdated. Procedures exist, but they may be ignored. The result is a slow accumulation of exposure that no audit is designed to catch. What HIPAA actually requires is something far more nuanced and continuous: a living, adaptive approach to identifying, mitigating, and documenting security risks as they evolve. The spirit of the Security Rule is not about conformance but responsiveness; not about static assurance, but active governance. And that begins with rethinking the entire security posture: not as a defensive perimeter, but as an exposure surface to be constantly reduced.
The real mandate: Deconstructing the HIPAA Security Rule
Behind the formalities of HIPAA lies a simple question: Do you know what could go wrong, and are you actively, demonstrably reducing the likelihood that it will? This is the animating force behind the Security Management Process (§164.308(a)(1)), a directive demanding both the identification of risks and the operational mechanisms to contain them on an ongoing basis. It’s not enough to acknowledge that threats exist; organizations must be able to demonstrate on an ongoing basis, with evidence, that they are systematically and competently reducing their exposure. The underlying message is clear: Keep doing your spadework, and keep the receipts.
This is why HIPAA splits the directive into two complementary functions: risk analysis and risk management. Risk analysis compels teams to uncover those latent exposures relevant to their specific infrastructure, workflows, and ePHI locations. Risk management then requires that those findings not remain as static reports, but directly inform prioritized remediation efforts.
Crucially, HIPAA does not dictate how this should be done. That flexibility is intentional. The framework is purposely technology-neutral, which enables organizations to adopt whichever tools and strategies best suit their function(s). With this interpretive latitude, however, comes an obligation: to continuously show that choices made in tooling or policy are measurably reducing risk. HIPAA allows freedom, but it demands accountability.

Anatomy of a breach: Common vulnerability exposures
The term “vulnerability exposure” is situational. A vulnerability becomes an exposure the moment it is left unaddressed in a system that handles ePHI. The longer it goes unresolved, the more it evolves from a latent defect into a probable breach vector. No actual breach or other evidence of intrusion is required for HIPAA to consider this a violation; the existence of preventable exposure is, itself, a failure of duty.
Some of the most devastating breaches in healthcare have stemmed from vulnerabilities that were well-known and widely documented. One of the largest for-profit hospital networks in the U.S., Community Health Systems (CHS), was breached in 2014 when attackers exploited the recently disclosed Heartbleed vulnerability in OpenSSL. This flaw allowed the exfiltration of encrypted ePHI data that included 4.5 million patients’ names, birth dates, and Social Security numbers. The incident occurred shortly after the patch was released, highlighting how attackers often strike before organizations can apply updates.
Other exposures are less visible, but equally dangerous. Flat network architectures with poor segmentation allow attackers more lateral movement once a single system is compromised. Misconfigured cloud storage, use of default credentials, or publicly exposed remote access ports all quietly increase the blast radius of any intrusion.
There are also the legacy protocols (e.g. TLS 1.0, SSLv3, old FTP variants) that persist in many clinical systems for reasons of compatibility or convenience. These are known weak points, ripe for interception or manipulation; their continued use signalling technical debt as well as critical strategic neglect.
These patterns highlight what makes exposure so dangerous in practice:
- Invisibility of exposure: Systems can appear operational and compliant while silently harboring risk, or worse, might already be a Trojan horse in your stronghold.
- Exploitation is optional: Breach consequences begin the moment attackers can access anything, not just when they manage to exfiltrate.
- Neglected fundamentals cause real damage: It’s rarely a zero-day; breaches more often employ known but untreated exploits.

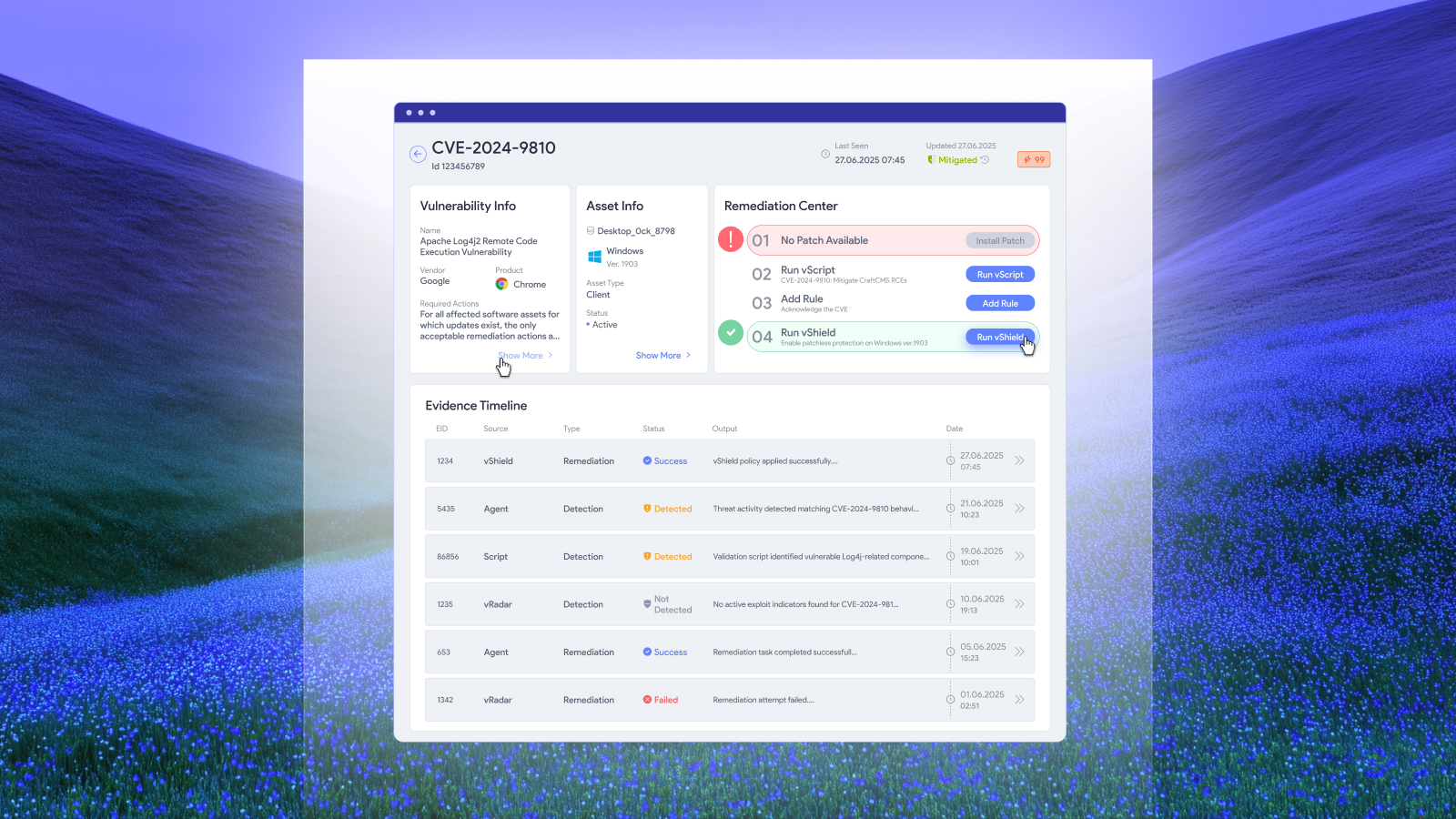
The proactive solution: The vulnerability management lifecycle
True compliance is not the absence of incidents; it’s the presence of a repeatable process for reducing exposure. The vulnerability management lifecycle transforms abstract HIPAA obligations into concrete, observable practice. The fundamentals matter: good network segmentation configuration alone can function like a series of blast walls, containing the severity of breaches. Instead of defending a perimeter, beyond merely shrinking your attack surface, pursuing resiliency in your vulnerability management design also sometimes means assuming that you’ve been breached already. The goal is now to shrink the blast radius systematically, continuously, and visibly.
Asset discovery and visibility
It begins with visibility. You cannot secure what you don’t know you have. That includes not just workstations and servers, but IoT devices, legacy systems, embedded clinical software, cloud workloads, and vendor-managed assets. Asset discovery must be systemic and dynamic, constantly updated through scanning, inventory tools, and endpoint telemetry - ideally as a matter of automated I[o]T device deployment and maintenance policy, ensuring actual provable security as well as reducing the technical labor load requirement on often-overworked and -underfunded IT departments in the medical sphere.
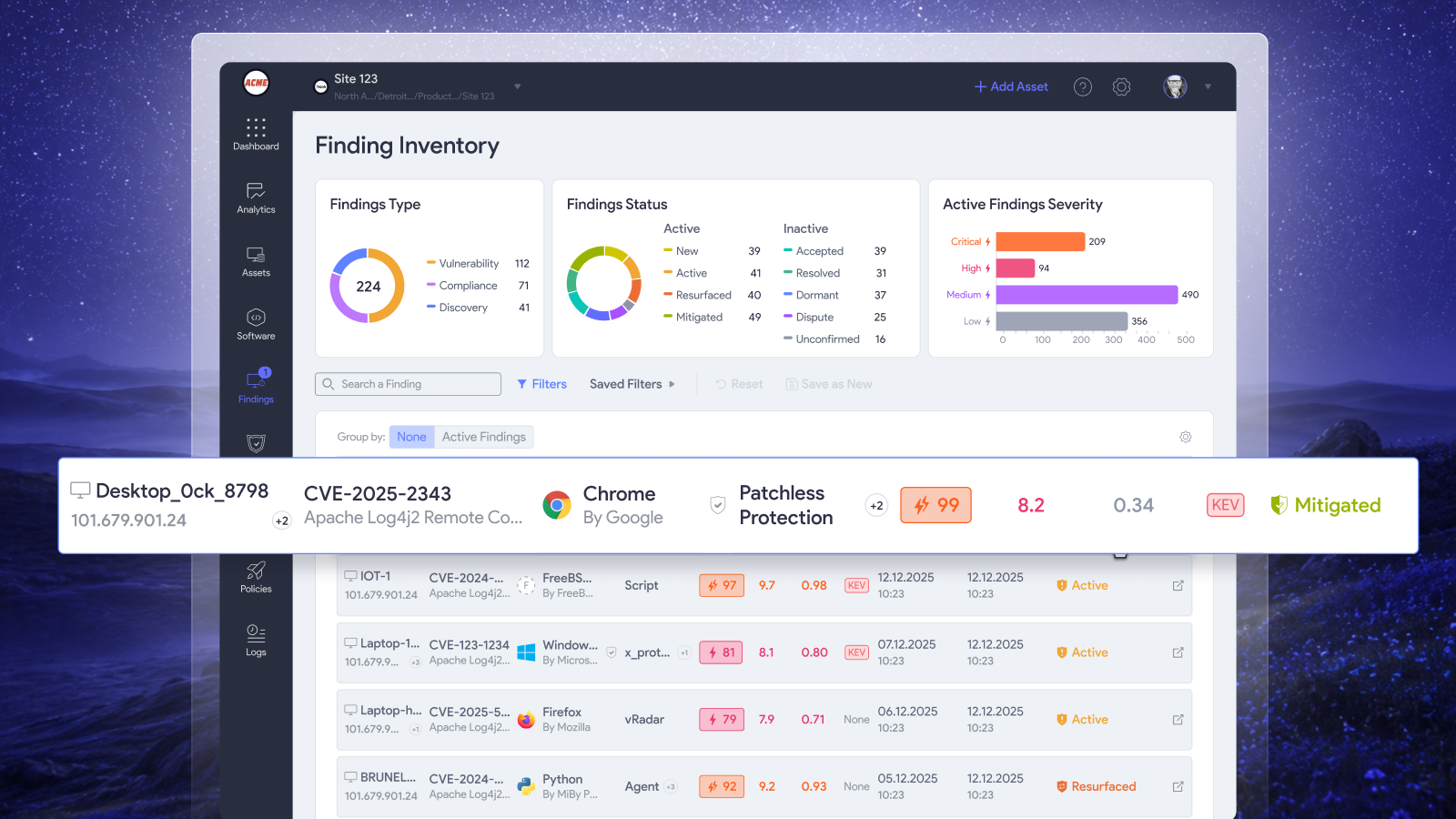
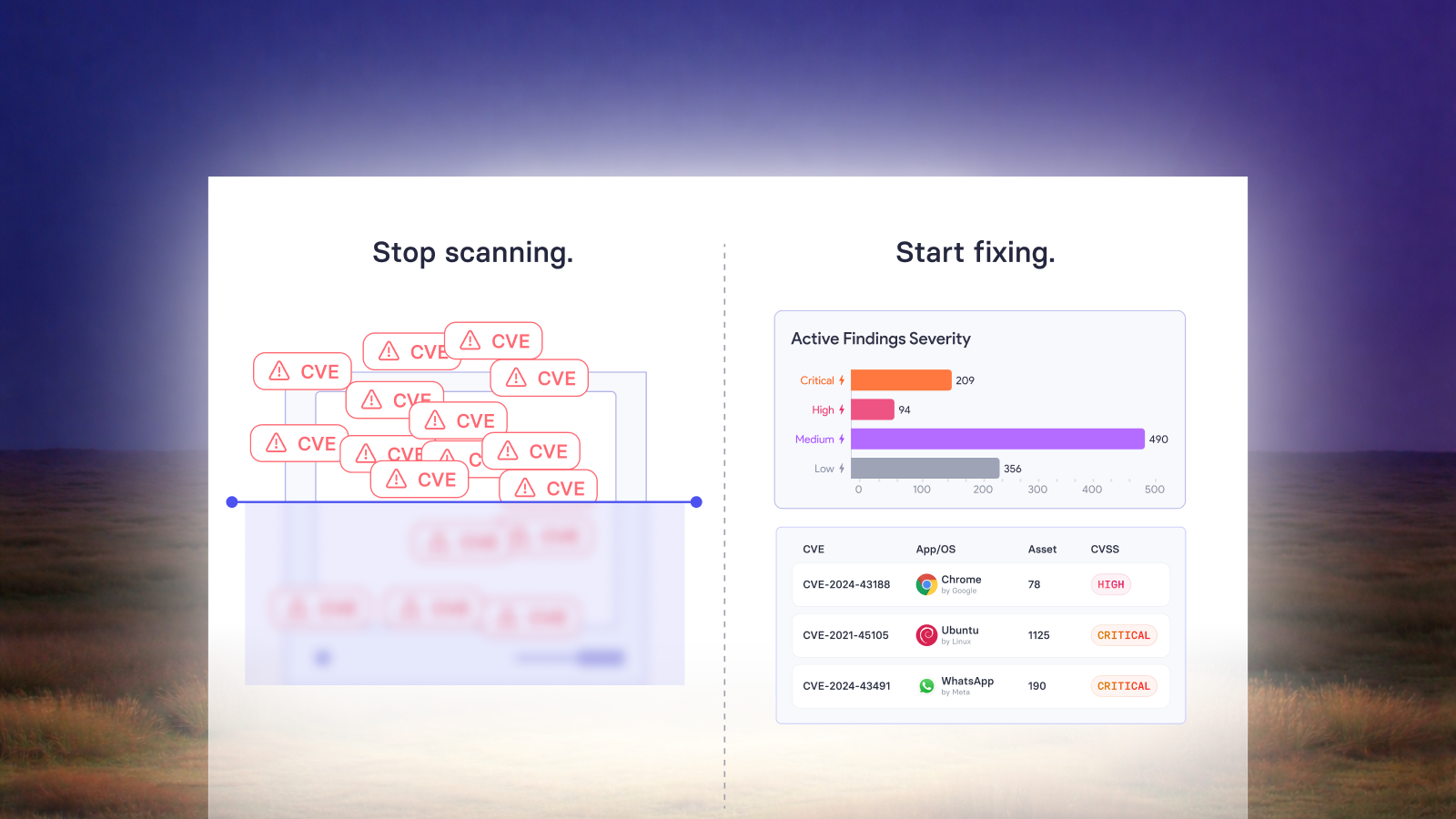
Continuous scanning for vulnerabilities
From there, organizations must identify vulnerabilities through regular, automated scanning. The emphasis is on cadence and coverage. A quarterly scan is not enough; risk changes weekly, even daily. Exploits can be discovered by lunchtime and be on dark web exploit marketplaces by dinner. Scanning must also extend beyond CVE lookups to detect misconfigurations, unauthorized services, and exposed ports.
Risk-based prioritization
Modern programs must therefore, of necessity, triage findings based not only on CVSS scores but on context. This includes:
- Business criticality: How essential is the asset to care delivery or system continuity?
- Data proximity: Does it handle or store regulated data directly?
- Exploit likelihood: Are there working exploits in the wild?
- Network location: Is the asset externally reachable or internally flat?
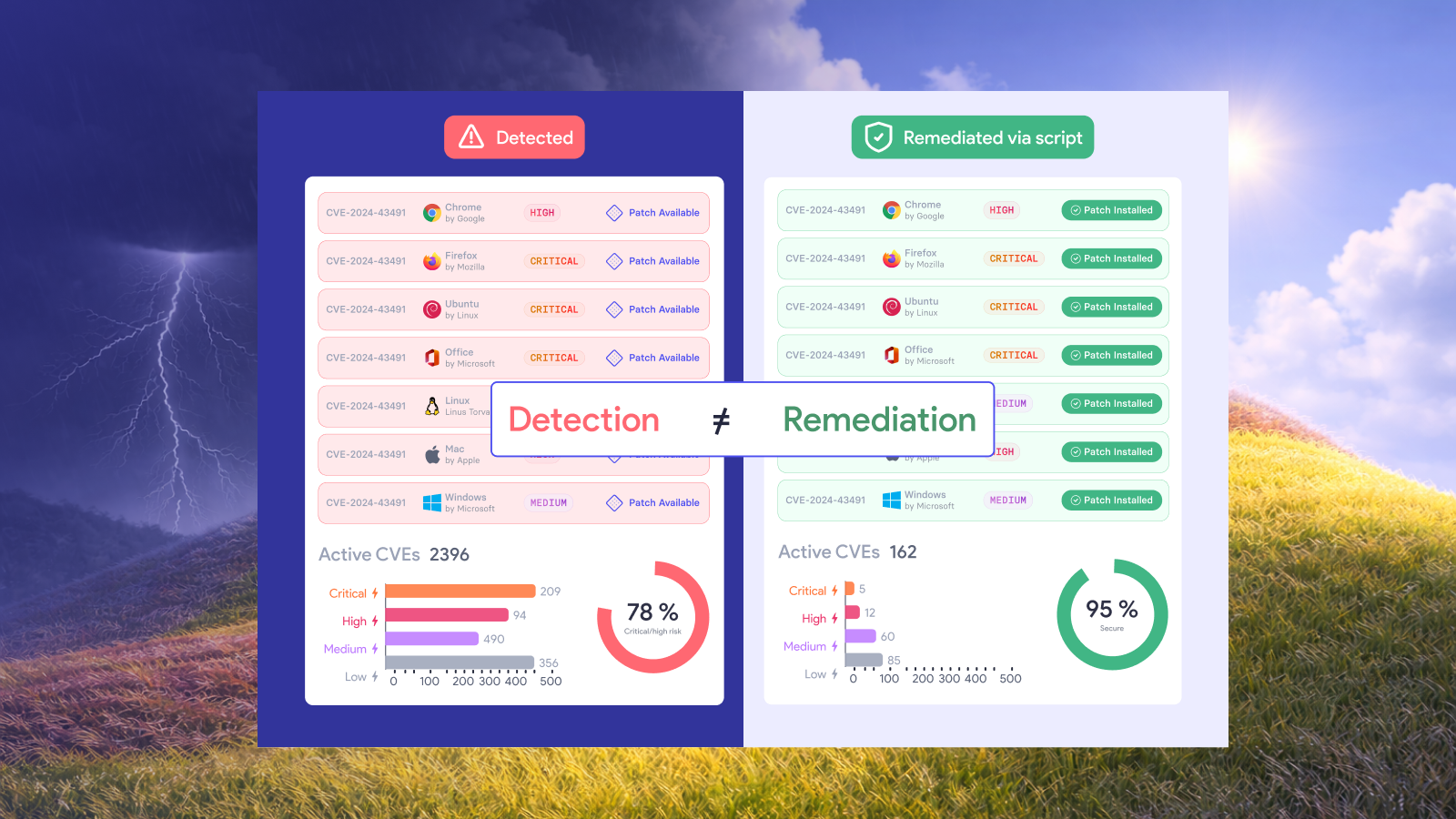
Remediation and risk acceptance
Whether patching, reconfiguring, or isolating, remediation must follow with an urgency commensurate with the risk. Not all risks can be resolved immediately, however; where necessary, formal risk acceptance processes must be invoked with justification, expiration timelines, and reviews.
Post-remediation validation
Post-remediation validation is not a luxury but rather quite essential. Scans must verify that changes are effective and persistent. Continuous monitoring then keeps drift and regression in check, ensuring that yesterday’s fixes remain today’s protections, and inform tomorrow’s proactivity. In the cybersecurity arms race, sometimes the cost of countering the enemy is thinking like the enemy
The cost of inaction: Lessons from HHS enforcement
HIPAA enforcement history is littered with examples of organizations penalized not for obscure failures, but for ignoring the obvious. At the University of Mississippi Medical Center (UMMC), years of inaction on known risks resulted in a $2.75 million fine. There were findings, there were warnings, but there was no meaningful response.
Large enterprises are not immune
Anthem Inc. offers another dubiously shiny example: a large, resource-rich enterprise fined $16 million after neglecting basic safeguards like enterprise-wide risk analysis. The breach exposed nearly 80 million records, evidence that even the best-funded organizations are not immune to foundational oversights.
Even small practices are not exempt
Even small practices are expected to act. Phoenix Cardiac Surgery was fined $100,000 not because it suffered a sophisticated attack, but because it failed to implement documented access controls and risk assessments. Size is not an exemption, merely a context.
Common enforcement themes
- Documenting without acting invites liability: It’s not enough to have a policy; regulators want proof of action.
- Known risk carries the heaviest penalty: You don’t need to be perfect, but you do need to be responsive.
- Compliance is no shield when the record shows negligence: Enforcement is retrospective and unforgiving.
Closing the leadership gap between compliance and control: From reactive to resilient
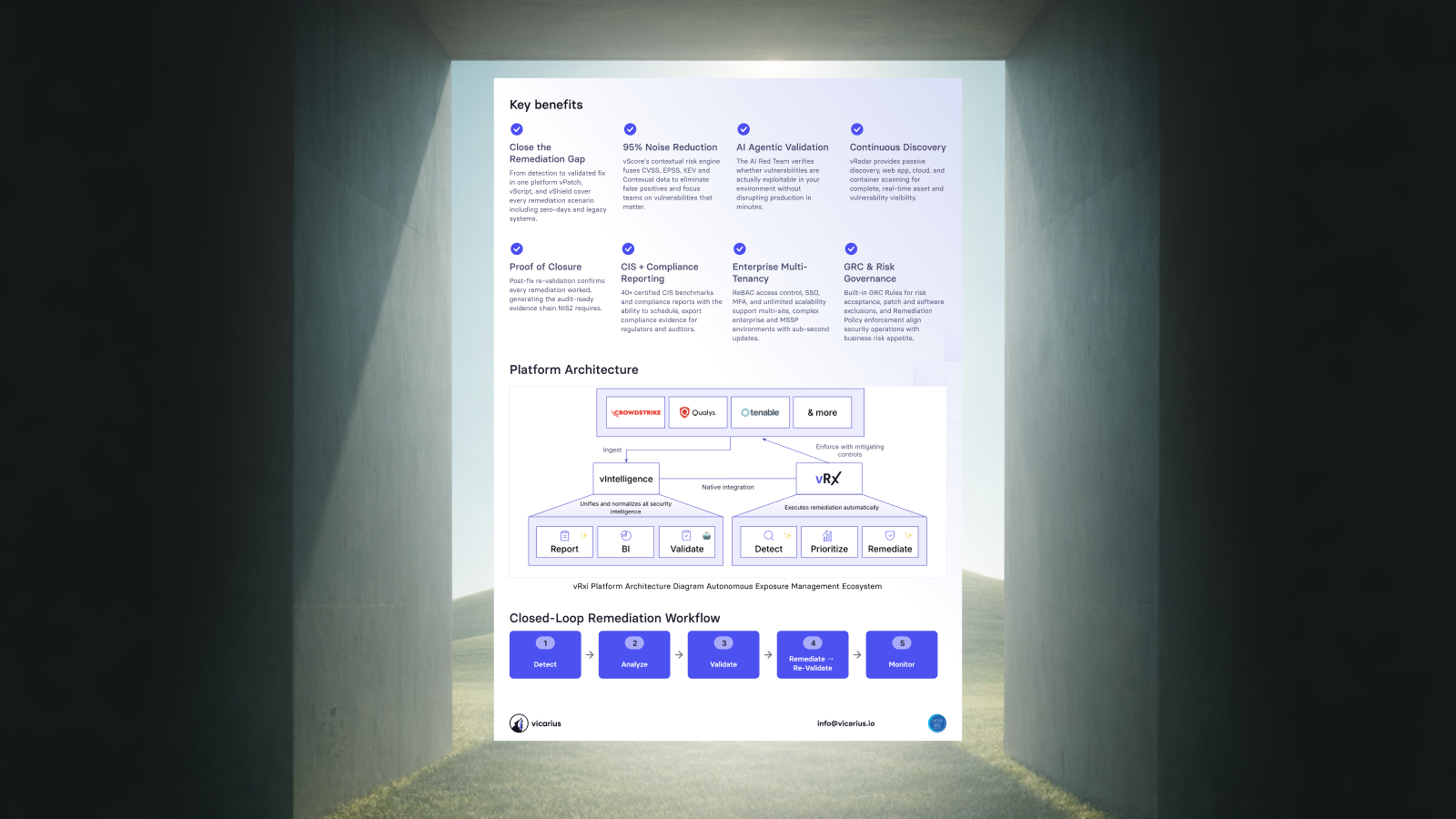
Breach recovery is no longer enough. What is needed now is operational resilience: the ability to reduce the likelihood of compromise, limit its scope when it happens, and to contain its cost. Proactive vulnerability management plays a central role in that shift, not only through technical remediation, but by creating traceable evidence of ongoing effort. It turns exposure into a measurable, manageable, demonstrably-duly-diligent defensible control. Regulators and insurers increasingly look for signs of operational maturity, not just paper compliance. These signals are hard to fake and easy to verify.
No organization reaches that point without leadership, however. CIOs, CISOs, and IT directors must shift the culture from compliance theatre to exposure reduction. That means supporting transparency, prioritizing risk over optics, and funding improvements that are about more than just looking good on audit day. The real test isn’t whether you can pass inspection. It’s whether your systems can withstand impact and whether your efforts stand up to scrutiny.
Request a demo today to see how the agentic AI in vRx by Vicarius can help you achieve true resilience.










.png)



























%20Signals%20a%20New%20Era%20of%20Supply%20Chain%20Risk.png)







.png)

















%20to%20Reduce%20Attack%20Surface.avif)



.avif)